The report also tracks a set of indicators outlined in the Roll Back Malaria (RBM) advocacy plan, Action and investment to defeat malaria 2016–2030 (AIM) (2) and the Sustainable Development Goals (SDGs) (3) – a set of interconnected global goals seen as a plan of action for people, the planet and prosperity (Fig. 1.2). The report highlights the various ways investment in the fight against malaria contributes to the SDGs and the aligned WHO “triple billion” targets of the 13th General programme of work (GPW13) (4) (Fig. 1.3)

Globally, new HIV infections among young women aged 15–24 years were reduced by 25% between 2010 and 2018. This is good news, but of course it remains unacceptable that every week 6000 adolescent girls and young women become infected with HIV. The sexual and reproductive health and rights of women and young people are still too often denied.
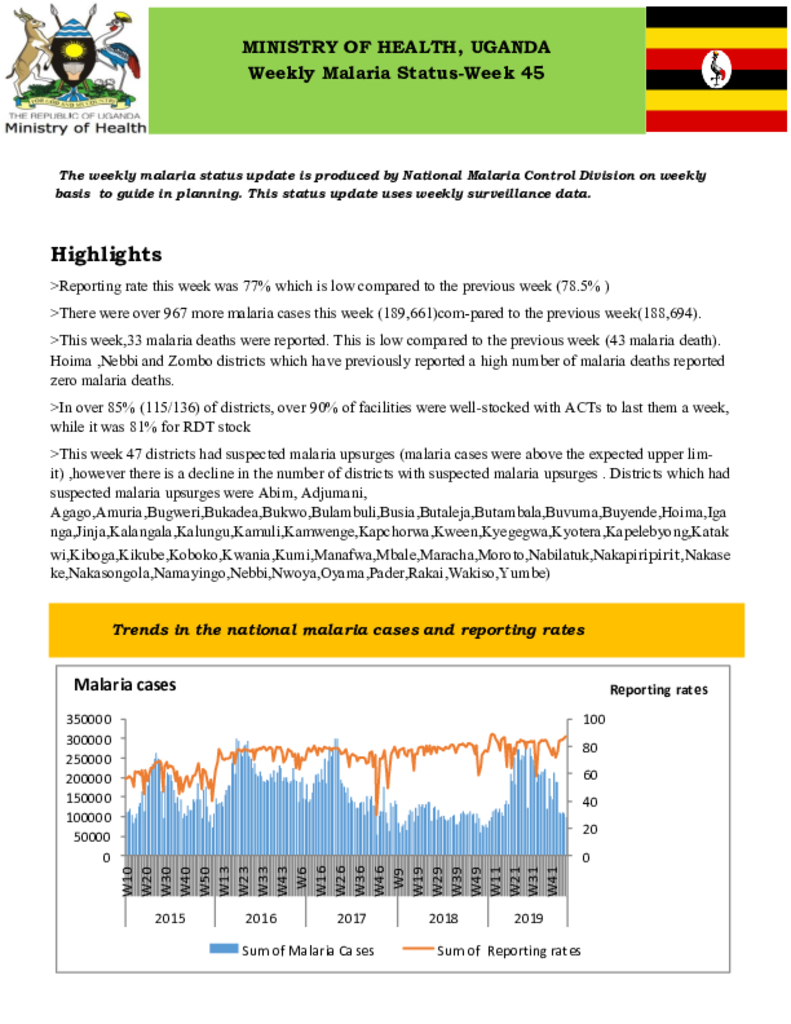
Reporting rate this week was 77% which is low compared to the previous week (78.5% ) There were over 967 more malaria cases this week (189,661)com-pared to the previous week(188,694).This week,33 malaria deaths were reported. This is low compared to the previous week (43 malaria death). Hoima ,Nebbi and Zombo districts which have previously reported a high number of malaria deaths reported zero malaria deaths. In over 85% (115/136) of districts, over 90% of facilities were well-stocked with ACTs to last them a week, while it was 81% for RDT stock This week 47 districts had suspected malaria upsurges (malaria cases were above the expected upper limit) ,however there is a decline in the number of districts with suspected malaria upsurges . Districts which had suspected malaria upsurges were Abim, Adjumani ,Agago ,Amuria, Bugweri, Bukadea, Bukwo, Bulambuli, Busia, Butaleja, Butambala, Buvuma, Buyende, Hoima, Iganga, Jinja, Kalangala, Kalungu, Kamuli, Kamwenge, Kapchorwa, Kween, Kyegegwa, Kyotera, Kapelebyong, Katakwi, Kiboga, Kikube, Koboko, Kwania, Kumi, Manafwa, Mbale, Maracha, Moroto, Nabilatuk, Nakapiripirit, Nakaseke, Nakasongola, Namayingo, Nebbi, Nwoya, Oyama, Pader, Rakai, Wakiso, Yumbe)
This issue focuses on the first quarter of 2019/2020 financial year. The aim of this bulletin is to inform district, national, and global stake-holders on progress achieved and challenges encountered in malaria control and reduction in Uganda. Most importantly, it is to encourage use of this information at all levels in order to foster improvement of our efforts and to high-light achievements and create awareness for increased resource mobilization & allocation in order to maintain the gains we have achieved.
The TWOS report for the period August- September 2019, summarizes facility reporting rates, timeliness of submission, patient numbers, estimates of stock status and central warehouse order fulfilment rates. It provides recommendations and actions to be taken by various stakeholders to mitigate supply issues
Facility reporting rates are calculated based on the total number of active ART facilities as of 1st October 2019. An ART facility is considered active if it submitted at least one order and or report in the last twelve months. The reporting rates for this cycle were 99% for PNFP facilities, 90% for PFP facilities and 93% for the government facilities.
Despite marked advancement in prevention, care and treatment, HIV in Uganda continues to exert severe constraints on the public health and economic well-being of a sizeable proportion of the population. The type of HIV epidemic in Uganda is described as severe, mature, and generalized but with sub-epidemics in different key, priority and other populations. Key populations are described by WHO and UNAIDS as those populations which are at higher risk for HIV irrespective of the epidemic type or local context and which face social and legal challenges that increase their vulnerability

This year’s global TB report reveals that countries are making progress. About 7 million people were reported to have been reached with quality TB care in 2018, up from 6.4 million in 2017. In addition, TB-related deaths dropped from 1.6 million in 2017 to 1.5 million in 2018. However, TB remains the top infectious killer worldwide, with 10 million people falling ill with TB in 2018. Although some countries are significantly accelerating
This TB and Leprosy Management Desk Guide is produced by the Ministry of Health National Tuberculosis and Leprosy Programme based on current Tuberculosis and Leprosy guidelines and field implementation experiences. The flip chart is intended to support the roll out of updated guidelines and serve as a reference guide for health workers on the management and control of TB and Leprosy at both facility and community level. It has been simplified for easy understanding by the frontline health workers to offer client centred TB and Leprosy services.
The evaluation targeted patients seen at Health Center IV (HCIV), General Hospitals, Regional and National Referral hospitals from the twelve health regions of MoH. A total of 158 health facilities were sampled for the evaluation, of which 116 were Health Center IVs, 22 were General Hospitals, 14 were Regional Referral Hospitals and 6 were National Referral Clinics. In each of the visited health facilities, records of TB and HIV patients for the two-time periods of July 01, 2012- June 30, 2013 and July 01, 2015-June 30, 2016 were abstracted
The survey established that DS-TB patients spent on average 369 United States dollars (USD) on TB related care per episode while MDR-TB patients spend on average 3722 USD. In the prediagnosis period, major cost drivers for both types of TB were medical and travel costs with both costs being higher for MDR-TB than DS-TB. In post diagnosis period, the major cost drivers for MDR-TB were nutritional supplements, travel and food while for DS-TB patients in the same period the main cost drivers were nutritional supplements




