This case study focuses on malaria case management activities was implemented in Ssembabule District, Uganda, by Minnesota International HealthVolunteers (MIHV) during the second phase of a U.S. Agency forInternational Development (USAID)-funded Child Survival project (1996-2000).
This publication draws upon current guidelines and information documents issued by the World Health Organization (WHO), which provide more detailed guidance on implementation for each of the specific subject areas. The listed references are limited to key readings for implementation of programme activities and to texts that provide important additional background and supplementary information.
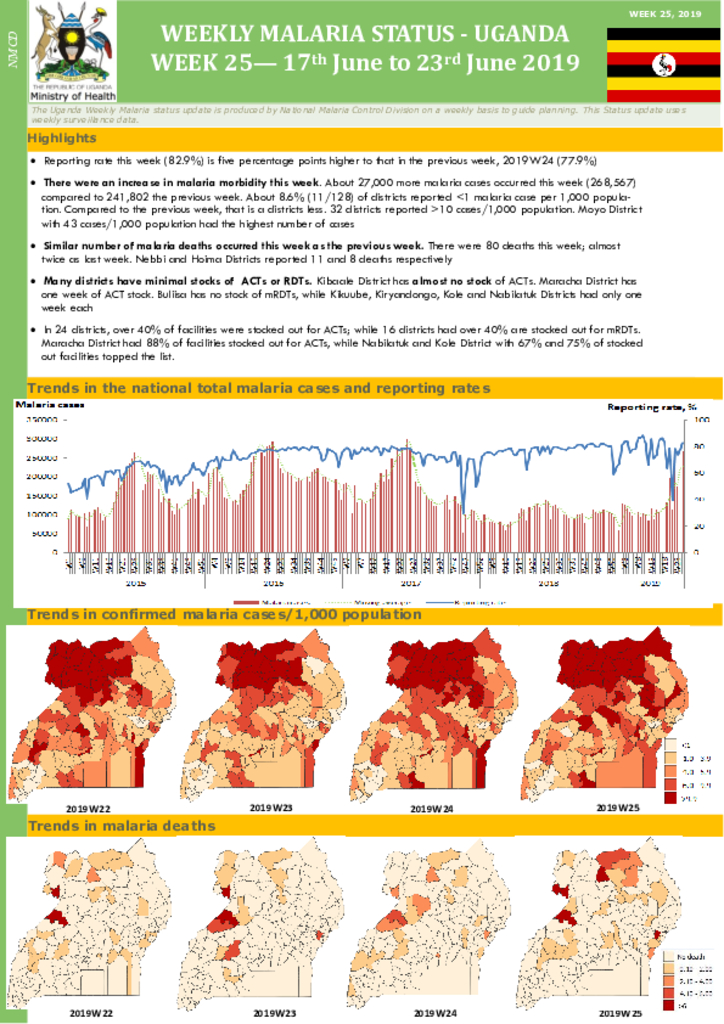
Reporting rate this week (82.9%) is five percentage points higher to that in the previous week, 2019W24 (77.9%) There were an increase in malaria morbidity this week. About 27,000 more malaria cases occurred this week (268,567) compared to 241,802 the previous week. About 8.6% (11/128) of districts reported <1 malaria case per 1,000 popula-tion. Compared to the previous week, that is a districts less. 32 districts reported >10 cases/1,000 population. Moyo District with 43 cases/1,000 population had the highest number of cases Similar number of malaria deaths occurred this week as the previous week.
There were 80 deaths this week; almost twice as last week. Nebbi and Hoima Districts reported 11 and 8 deaths respectively Many districts have minimal stocks of ACTs or RDTs. Kibaale District has almost no stock of ACTs. Maracha District has one week of ACT stock. Buliisa has no stock of mRDTs, while Kikuube, Kiryandongo, Kole and Nabilatuk Districts had only one week each In 24 districts, over 40% of facilities were stocked out for ACTs; while 16 districts had over 40% are stocked out for mRDTs. Maracha District had 88% of facilities stocked out for ACTs, while Nabilatuk and Kole District with 67% and 75% of stocked out facilities topped the list.
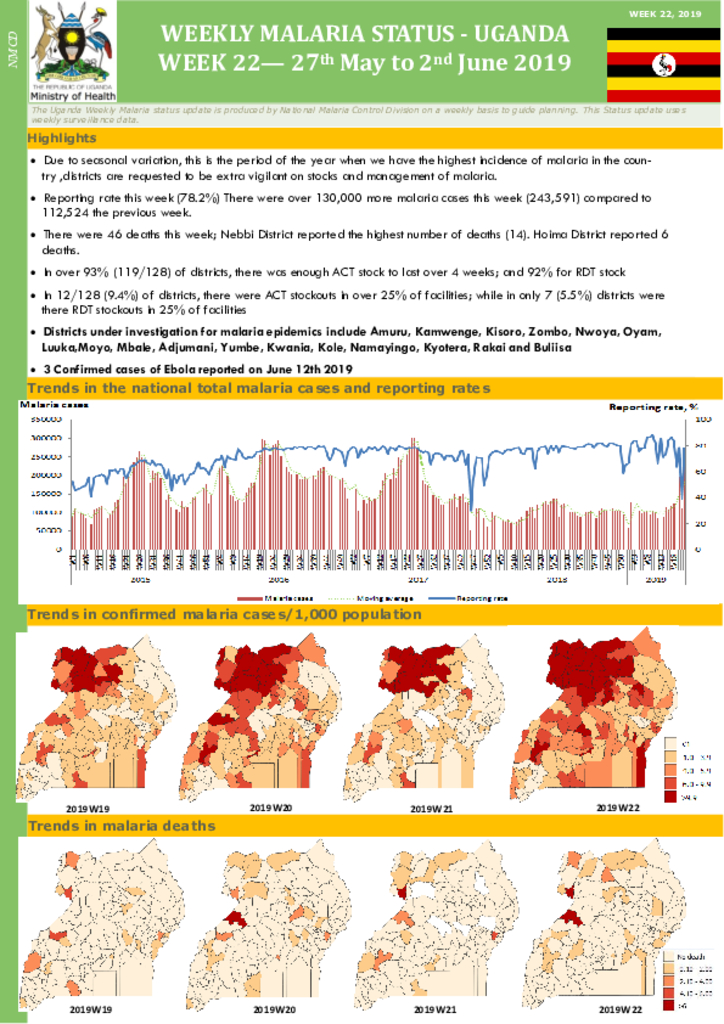
Due to seasonal variation, this is the period of the year when we have the highest incidence of malaria in the country
,districts are requested to be extra vigilant on stocks and management of malaria. Reporting rate this week (78.2%) There were over 130,000 more malaria cases this week (243,591) compared to 112,524 the previous week. There were 46 deaths this week; Nebbi District reported the highest number of deaths (14). Hoima District reported 6 deaths. In over 93% (119/128) of districts, there was enough ACT stock to last over 4 weeks; and 92% for RDT stock In 12/128 (9.4%) of districts, there were ACT stockouts in over 25% of facilities; while in only 7 (5.5%) districts were there RDT stockouts in 25% of facilities Districts under investigation for malaria epidemics include Amuru, Kamwenge, Kisoro, Zombo, Nwoya, Oyam, Luuka,Moyo, Mbale, Adjumani, Yumbe, Kwania, Kole, Namayingo, Kyotera, Rakai and Buliisa
3 Confirmed cases of Ebola reported on June 12th 2019
The HIV/AIDS epidemic is a global crisis and constitutes one of the most formidable obstacles towards sustainable development and social progress. In the most affected countries, the impact of HIV/AIDS poses a severe threat to every aspect of life, as it erodes decades of developmental gains and threatens the security by destabilizing the structure of societies and undermining their economies
Voluntary counselling and testing (VCT) is the process by which an individual undergoes counselling, enabling him or her to make an informed choice about being tested for HIV1. In recent years, voluntary HIV testing, in combination with pre- and post-test counselling, has
The survey fieldwork was conducted in forty six fishing communities of the Lake Victoria Basin of Uganda in August 2010. The main aim was to establish HIV prevalence among fishing communities, the associated drivers of risk and vulnerability; and the effectiveness of HIV and AIDS response.
The survey methods consisted of individual interviews, focus group discussions and key informants interviews. A desk-review was conducted to document HIV service availability and utilization, as well as institutional policies and structures for the coordination and delivery of HIV services. Laboratory testing for HIV was conducted both in the field and at central level.
HIV Counseling Supervision is a crucial component of any HIV/AIDS counseling or care and support service. It provides a way to support counselors and to address clients’ needs while at the same time upholding the professional practice of counseling around the globe. Supervision is an excellent opportunity to provide follow-up training, improve performance,and solve other systemic problems that may contribute to poor performance. Therefore,there is a continuing need, especially in developing countries, for “learning by doing” andfor documenting how well different concepts and practices translate across cultures and
settings.
HIV Counseling Supervision is a crucial component of any HIV/AIDS counseling or care and support service. It provides a way to support counselors and to address clients’ needs while at the same time upholding the professional practice of counseling around the globe. Supervision is an excellent opportunity to provide follow-up training, improve performance, and solve other systemic problems that may contribute to poor performance. Therefore, there is a continuing need, especially in developing countries, for “learning by doing” and for documenting how well different concepts and practices translate across cultures and settings.
This policy replaces the 2003 document, uganda national policy guidelines for HIV voluntary counselling and testing. The revision was promted by scientific and programmatic advances in HIv counselling and as well advances in prevention.
The fourth Millennium Development Goal (MDG) — to reduce by two-thirds, between 1990 and 2015, the under-five mortality rate — is ambitious, but achievable. Currently, more than 10 million children under five die each year, four million of them in the first month. It is estimated that around two-thirds of these child deaths could be prevented by increasing coverage of a handful of existing, relatively low-tech and inexpensive interventions.
Promoting breastfeeding is key among these interventions. MDG 7 — to have halted by 2015 and begun to reverse the spread of HIV/AIDS — is also closely linked to this issue. Governments and donors must greatly increase their commitment and resources for implementation of the Global Strategy for Infant and Young Child Feeding and the United Nations (UN) HIV and Infant Feeding Framework for Priority Action in order to effectively prevent postnatal HIV infections, improve HIV-free survival and achieve the relevant global goals.
The 2014 Uganda HIV Country progress report was prepared through a consultative government led process involving all key players to give the status of the HIV response in 2014 and also met the Country’s reporting obligations to national and international commitments. The report details key milestones achieved in 2014 in the areas of prevention, treatment, care and support and systems strengthen as aligned to the ten Global HLM targets. Uganda being a signatory to a number of global pronouncements including the commitments in the 2011 UN Political Declaration on HIV and AIDS, the report will feed into the Global AIDS report for presentation to the UN General Assembly on the progress achieved in realising the commitments made in the declaration against the 2011 ten HLM targets.




