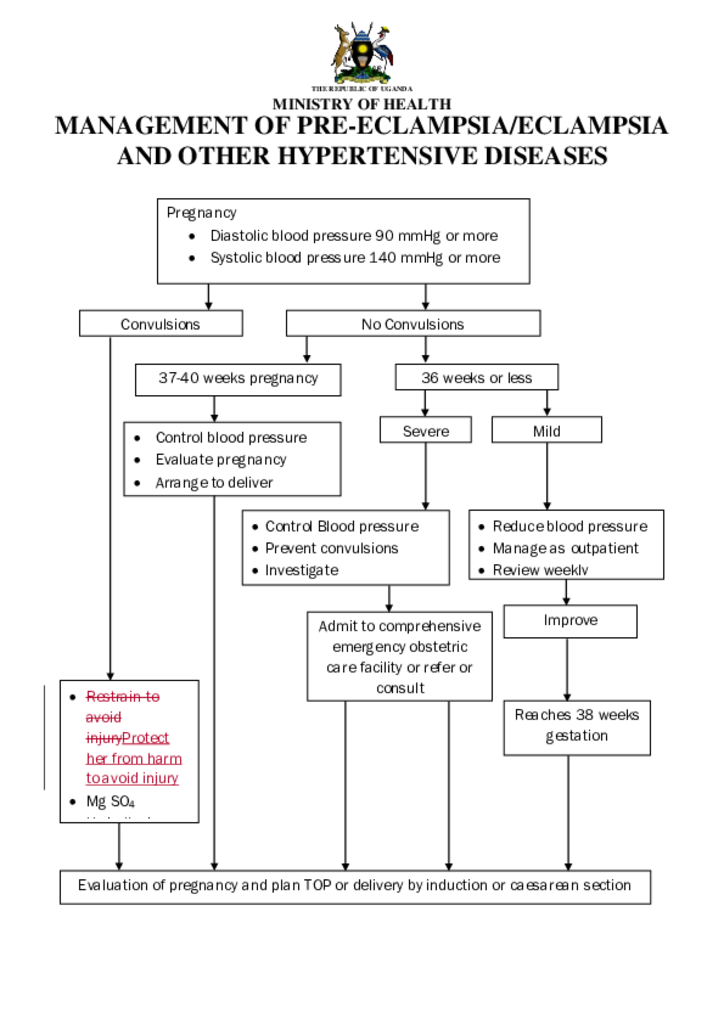
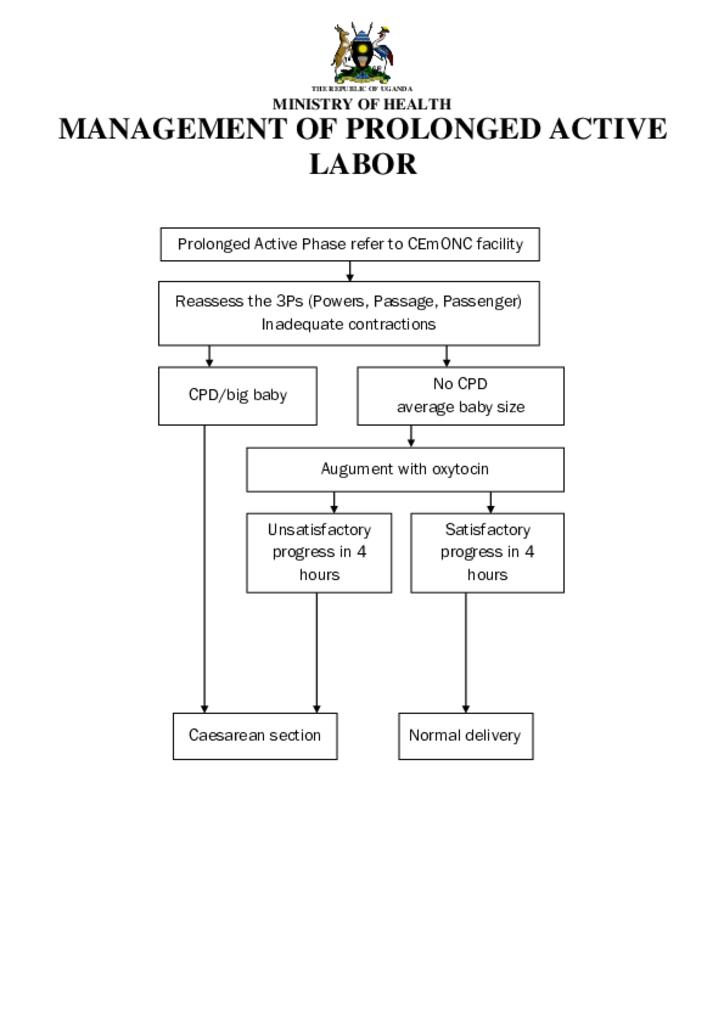
Management of Pre- Eclampsia /Eclampsia and Other Hypertensive Diseases
The aim of Pregnancy, childbirth, postpartum and newborn care guide for essential practice (PCPNC) is to provide evidence-based recommendations to guide health care professionals in the management of women during pregnancy, childbirth and postpartum, and post abortion, and newborns during their first week of life, including management of endemic diseases like malaria, HIV/AIDS, TB and anaemia.
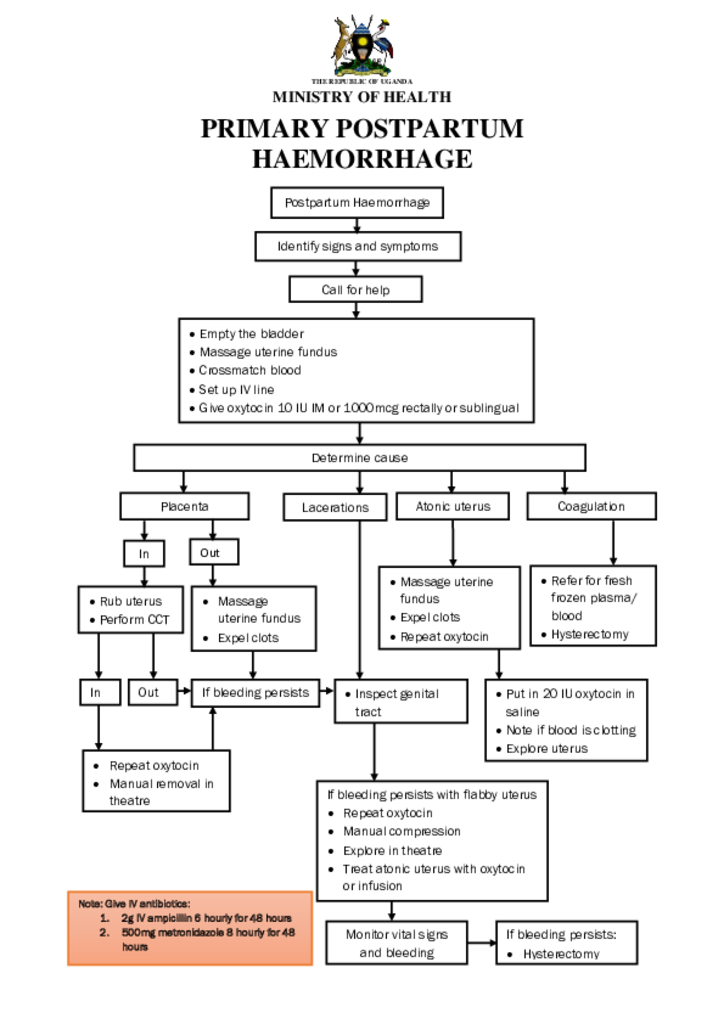
Primary Postpartum Haemorrhage
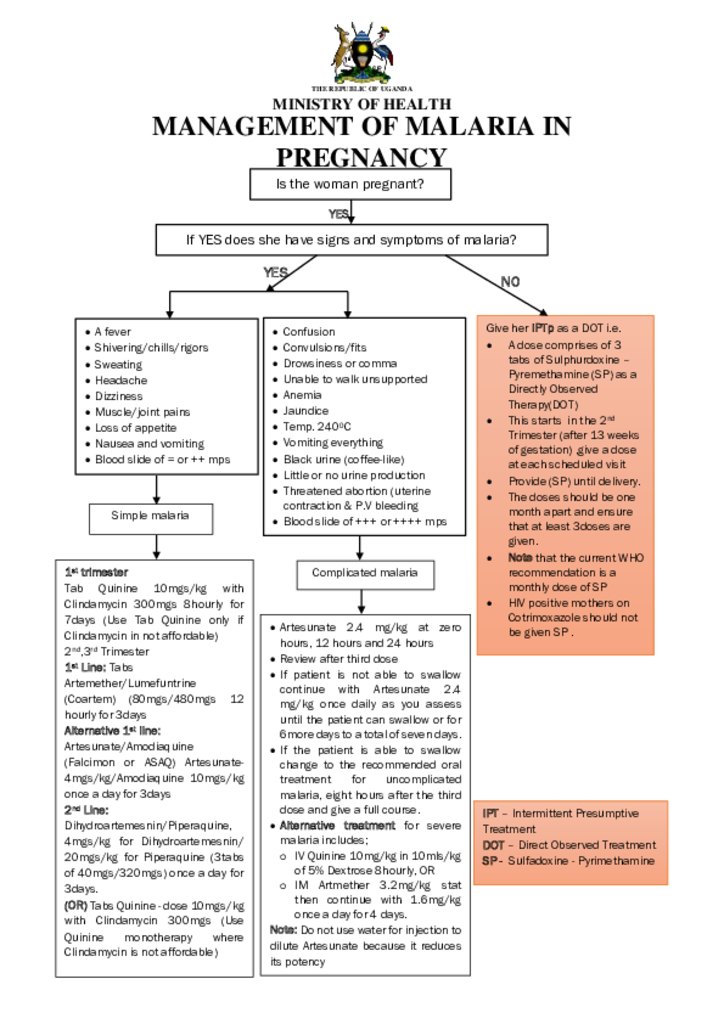
Management of Malaria in Pregnancy
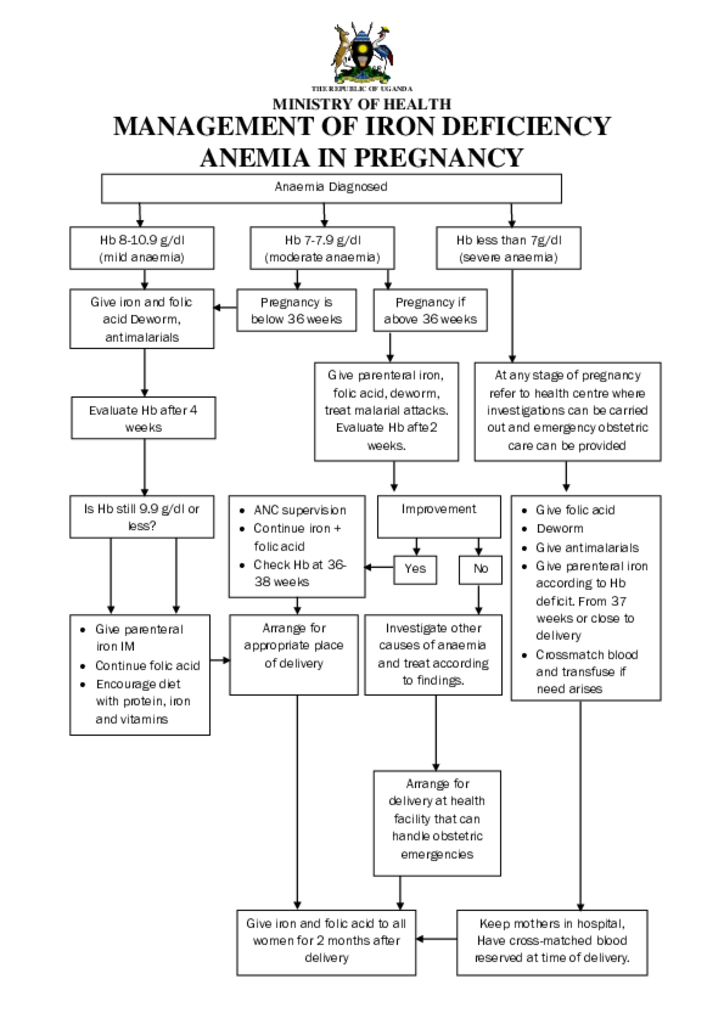
Management of Iron Deficiency Anemia Pregnancy
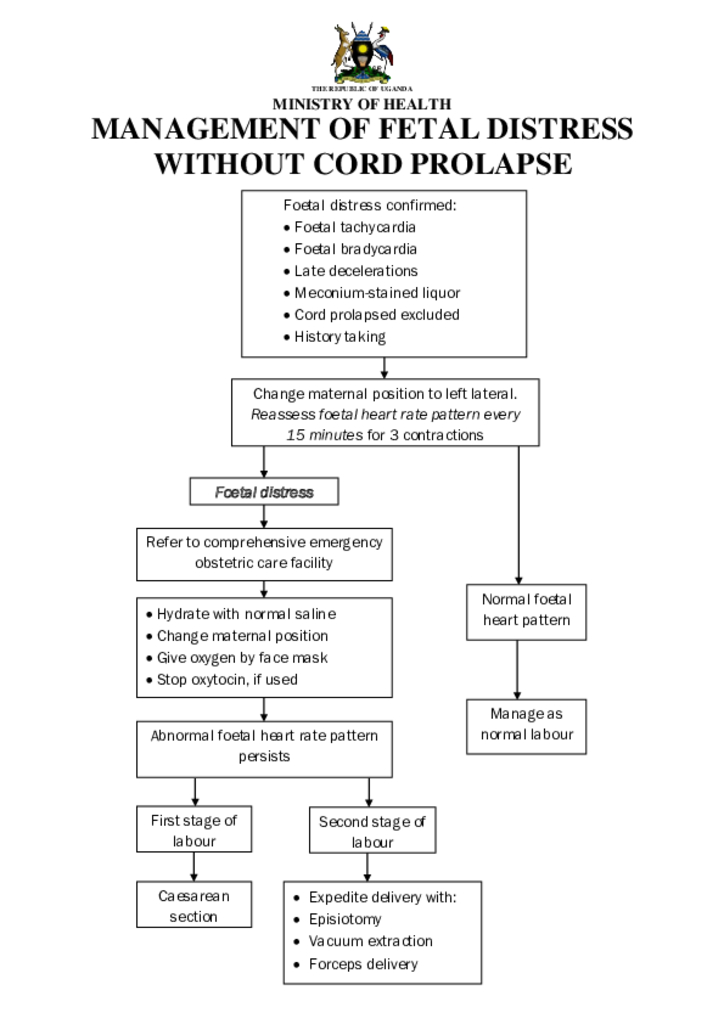
Management of Fetal Distress Without Cord Prolapse
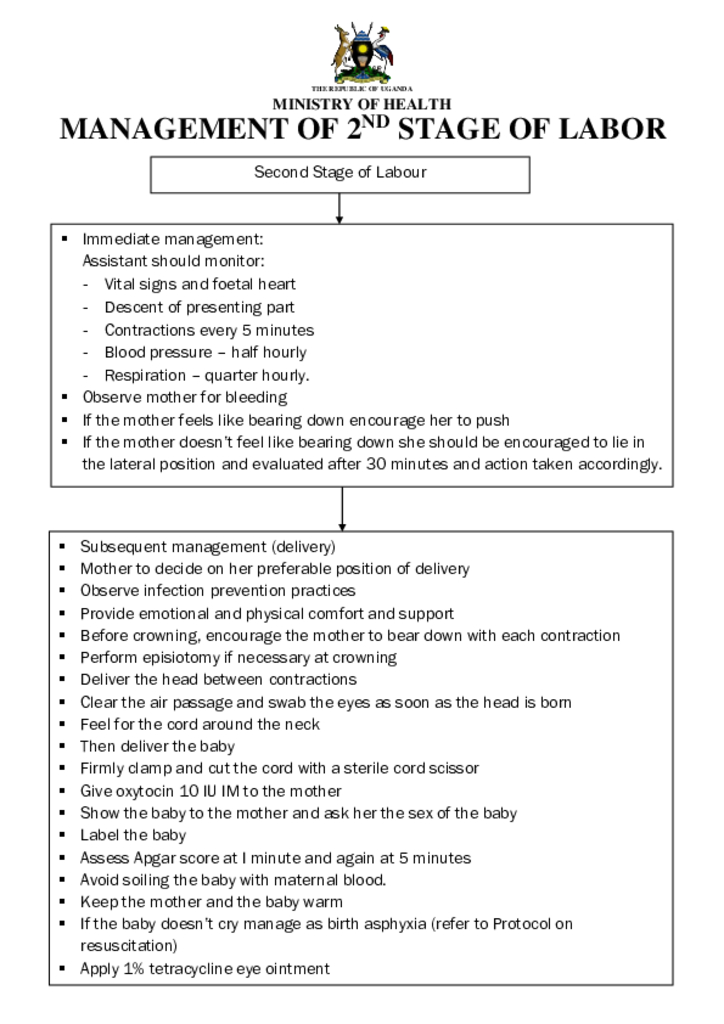
Management of 2nd stage of labor
Since the Cairo International Conference on Population and Development (ICPD program of Action 1994), global recognition of the importance of men’s involvement in Sexual and Reproductive Health and Rights (SRHR) has increased.
Issues such as the AIDS epidemic have reinforced the urgency of encouraging men to take responsibility for their own sexual and Reproductive Health and that of their partners (Salem, 2004). Despite global recognition at the level of international agreements, many countries have not developed large-scale programs that reach out to men.
As a result, many men are not aware of why they need to be involved in SRH, how they can be involved, and what services are available for them and their partners.
The last 15 years have witnessed increasing global recognition of the importance of men’s involvement in RMNCAH-N, GBV/VAC, SRHR including HIV/TB. The urgency of encouraging men to take responsibility for their own SRH and their partner’s is gaining momentum. However, Uganda has not developed large-scale programs that reach out to men.




