
The purpose of this report is to inform the Ministry of Health and all stakeholders of the stock levels in the country as a tool that enables appropriate logistics decision making. This report highlights stock status, real challenges, bottlenecks but also recommends potential solutions to mitigate stock outs and expiries of ARVs & HIV test kits, ACTs, Anti-TB medicines, Reproductive Health items, selected Laboratory commodities, Vaccines and selected medicines for treatment of Opportunistic Infections In the Republic of Uganda
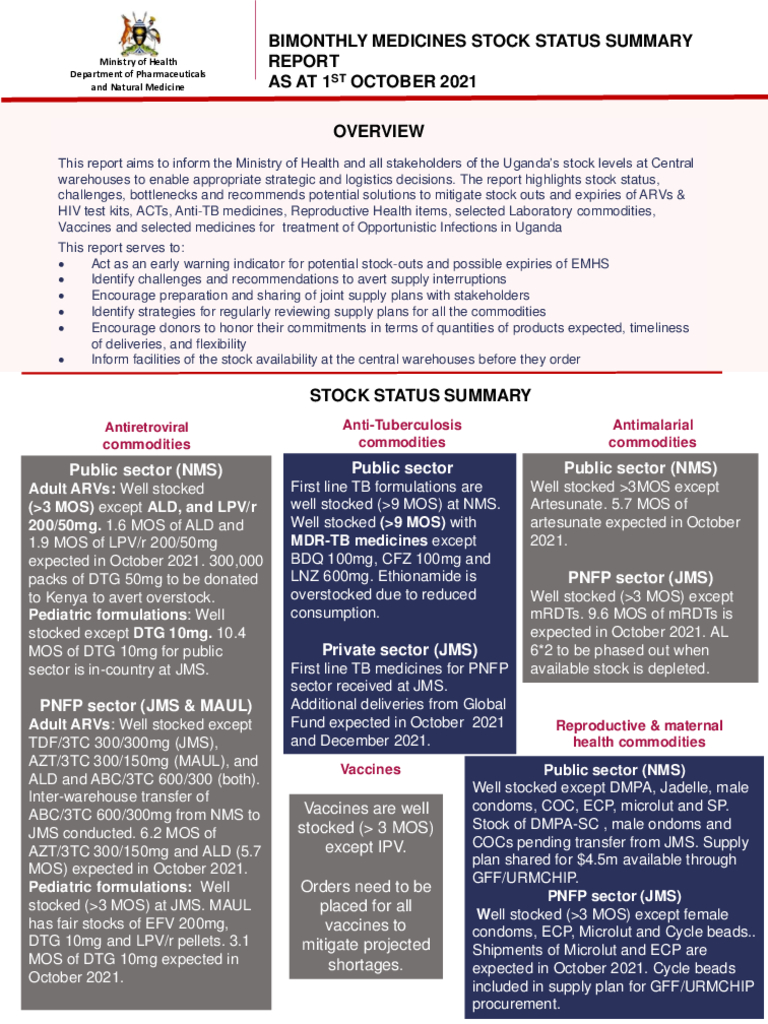
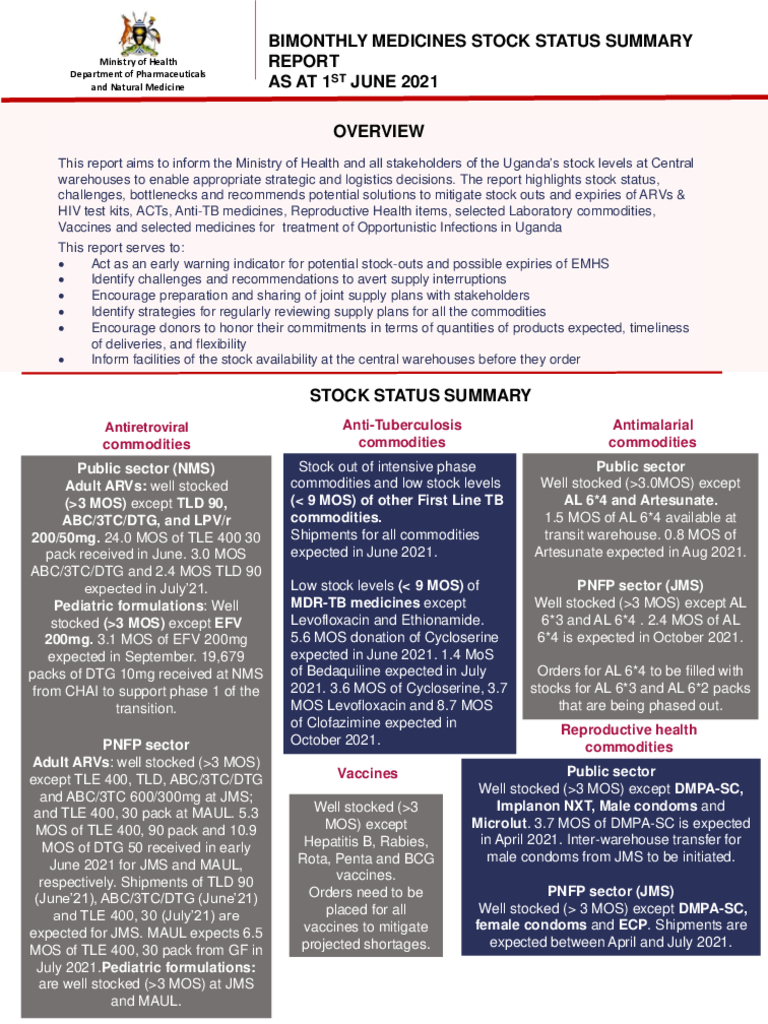
This report aims to inform the Ministry of Health and all stakeholders of the Uganda’s stock levels at Central warehouses to enable appropriate strategic and logistics decisions. The report highlights stock status, challenges, bottlenecks and recommends potential solutions to mitigate stock outs and expiries of ARVs & HIV test kits, ACTs, Anti-TB medicines, Reproductive Health items, selected Laboratory commodities, Vaccines and selected medicines for treatment of Opportunistic Infections in Uganda.

Antimicrobial resistance (AMR) has many drivers, with antibiotics use in the human and animal sectors being the most significant and modifiable factor. We all must work towards preservation of the available antimicrobials through judicious and thoughtful antimicrobial use in all sectors. All of us have a vita role to play by making meaningful decisions and changes that can improve the use antimicrobials, patient safety, and the health of the population.
This report aims to inform the Ministry of Health and all stakeholders of the Uganda’s stock levels at Central warehouses to enable appropriate strategic and logistics decisions. The report highlights stock status, challenges, bottlenecks and recommends potential solutions to mitigate stock outs and expiries of ARVs & HIV test kits, ACTs, Anti-TB medicines, Reproductive Health items, selected Laboratory commodities, Vaccines and selected medicines for treatment of Opportunistic Infections in Uganda.

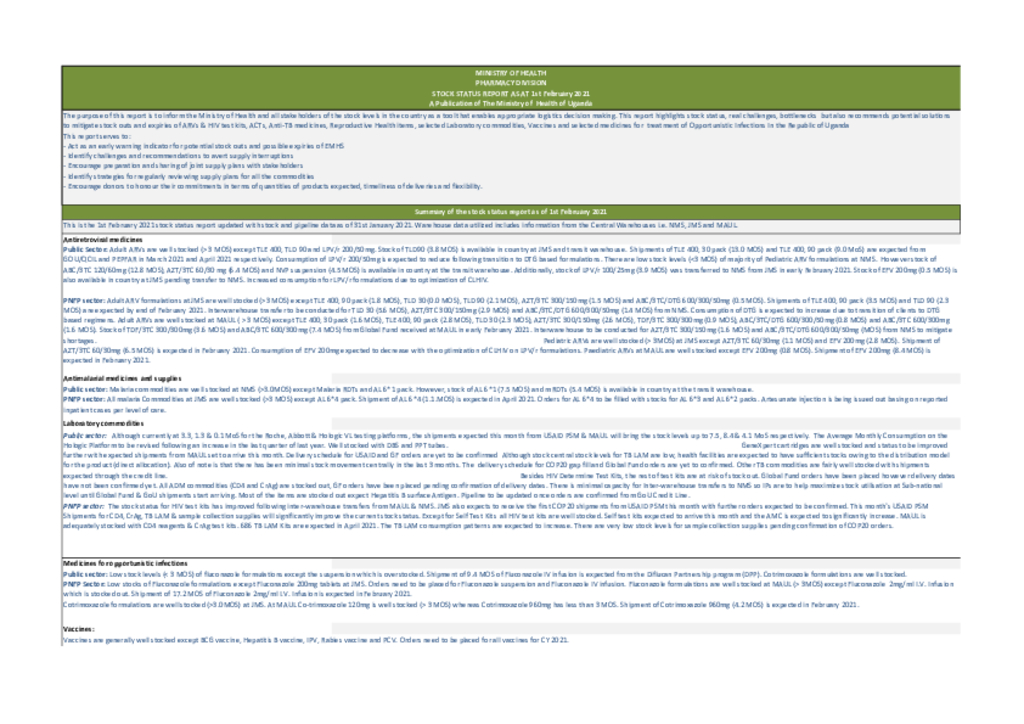
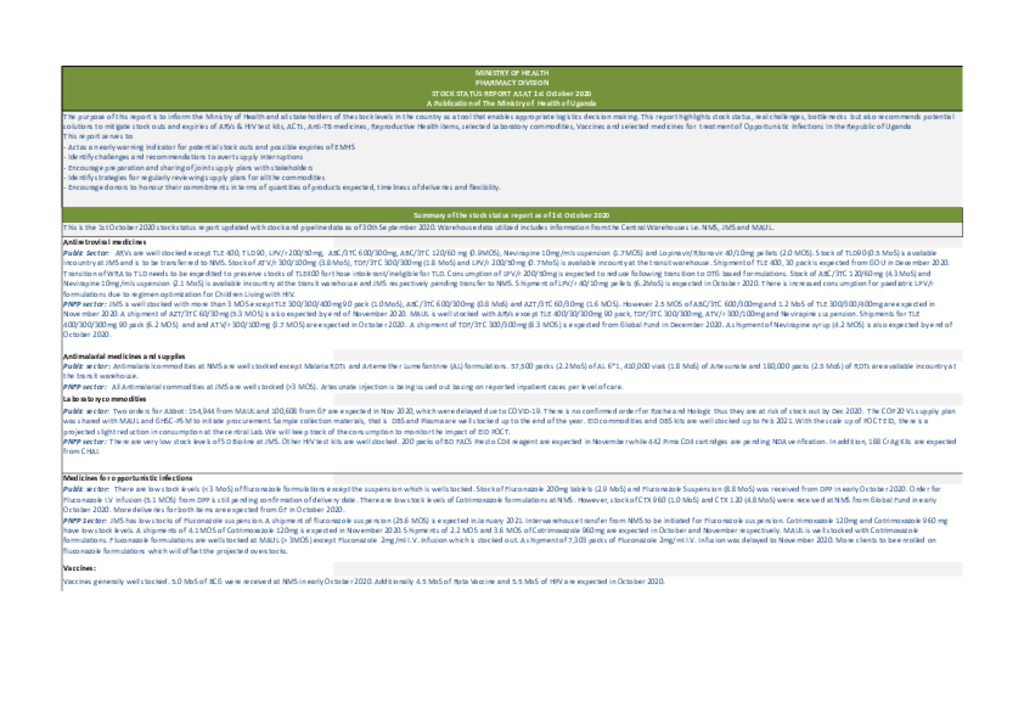
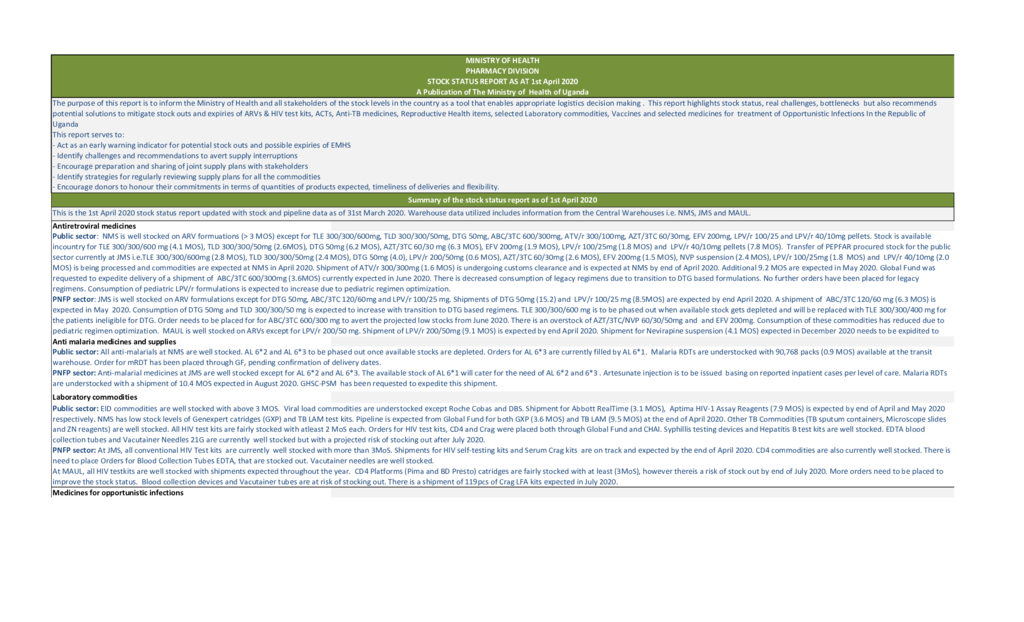
The purpose of this report is to inform the Ministry of Health and all stakeholders of the stock levels in the country as a tool that enables appropriate logistics decision making. This report highlights stock status, real challenges, bottlenecks but also recommends potential solutions to mitigate stock outs and expiries of ARVs & HIV test kits, ACTs, Anti-TB medicines, Reproductive Health items, selected Laboratory commodities, Vaccines and selected medicines for treatment of Opportunistic Infections In the Republic of Uganda This report serves to: - Act as an early warning indicator for potential stock outs and possible expiries of EMHS - Identify challenges and recommendations to avert supply interruptions - Encourage preparation and sharing of joint supply plans with stakeholders - Identify strategies for regularly reviewing supply plans for all the commodities - Encourage donors to honour their commitments in terms of quantities of products expected, timeliness of deliveries and flexibility - Inform facilities of the stock availability at the central warehouses before they orde
The second meeting of the WHO Strategic Advisory Group of Experts on In Vitro Diagnostics (SAGE IVD) was held on 18–22 March 2019 at WHO headquarters in Geneva, Switzerland.
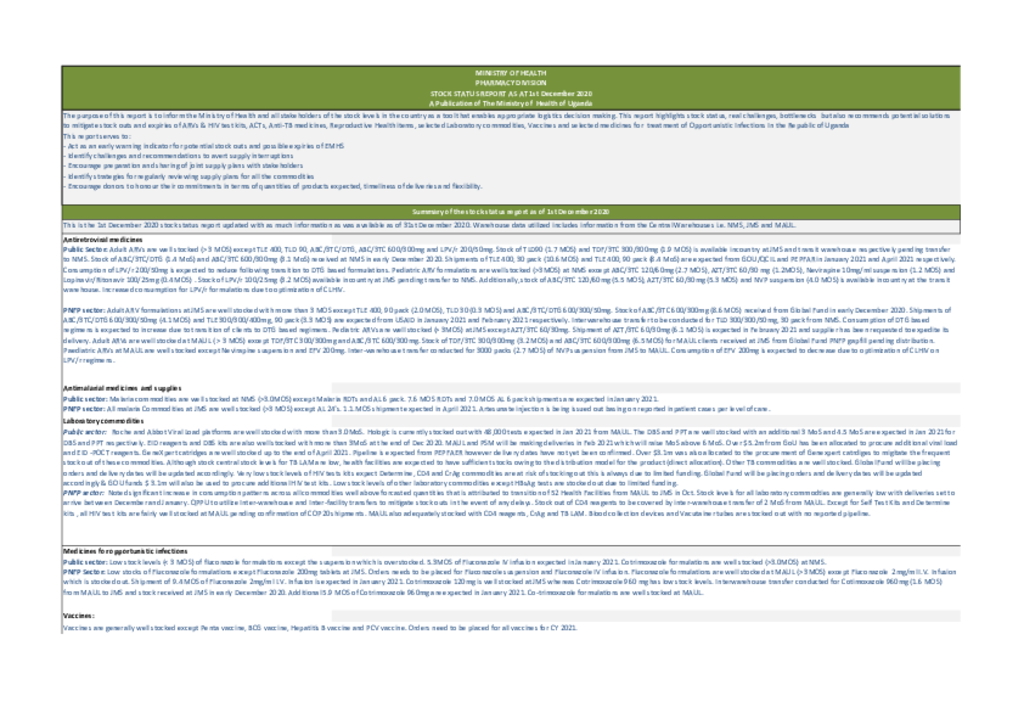
The purpose of this report is to inform the Ministry of Health and all stakeholders of the stock levels in the country as a tool that enables appropriate logistics decision making. This report highlights stock status, real challenges, bottlenecks but also recommends potential solutions to mitigate stock outs and expiries of ARVs & HIV test kits, ACTs, Anti-TB medicines, Reproductive Health items, selected Laboratory commodities, Vaccines and selected medicines for treatment of Opportunistic Infections In the Republic of Uganda This report serves to: - Act as an early warning indicator for potential stock outs and possible expiries of EMHS - Identify challenges and recommendations to avert supply interruptions - Encourage preparation and sharing of joint supply plans with stakeholders - Identify strategies for regularly reviewing supply plans for all the commodities - Encourage donors to honour their commitments in terms of quantities of products expected, timeliness of deliveries and flexibility.
The purpose of this report is to inform the Ministry of Health and all stakeholders of the stock levels in the country as a tool that enables appropriate logistics decision making. This report highlights stock status, real challenges, bottlenecks but also recommends potential solutions to mitigate stock outs and expiries of ARVs & HIV test kits, ACTs, Anti-TB medicines, Reproductive Health items, selected Laboratory commodities, Vaccines and selected medicines for treatment of Opportunistic Infections In the Republic of Uganda This report serves to: - Act as an early warning indicator for potential stock outs and possible expiries of EMHS - Identify challenges and recommendations to avert supply interruptions - Encourage preparation and sharing of joint supply plans with stakeholders - Identify strategies for regularly reviewing supply plans for all the commodities - Encourage donors to honour their commitments in terms of quantities of products expected, timeliness of deliveries and flexibility.
The purpose of this report is to inform the Ministry of Health and all stakeholders of the stock levels in the country as a tool that enables appropriate logistics decision making. This report highlights stock status, real challenges, bottlenecks but also recommends potential solutions to mitigate stock outs and expiries of ARVs & HIV test kits, ACTs, Anti-TB medicines, Reproductive Health items, selected Laboratory commodities, Vaccines and selected medicines for treatment of Opportunistic Infections In the Republic of Uganda This report serves to: - Act as an early warning indicator for potential stock outs and possible expiries of EMHS - Identify challenges and recommendations to avert supply interruptions - Encourage preparation and sharing of joint supply plans with stakeholders - Identify strategies for regularly reviewing supply plans for all the commodities - Encourage donors to honour their commitments in terms of quantities of products expected, timeliness of deliveries and flexibility
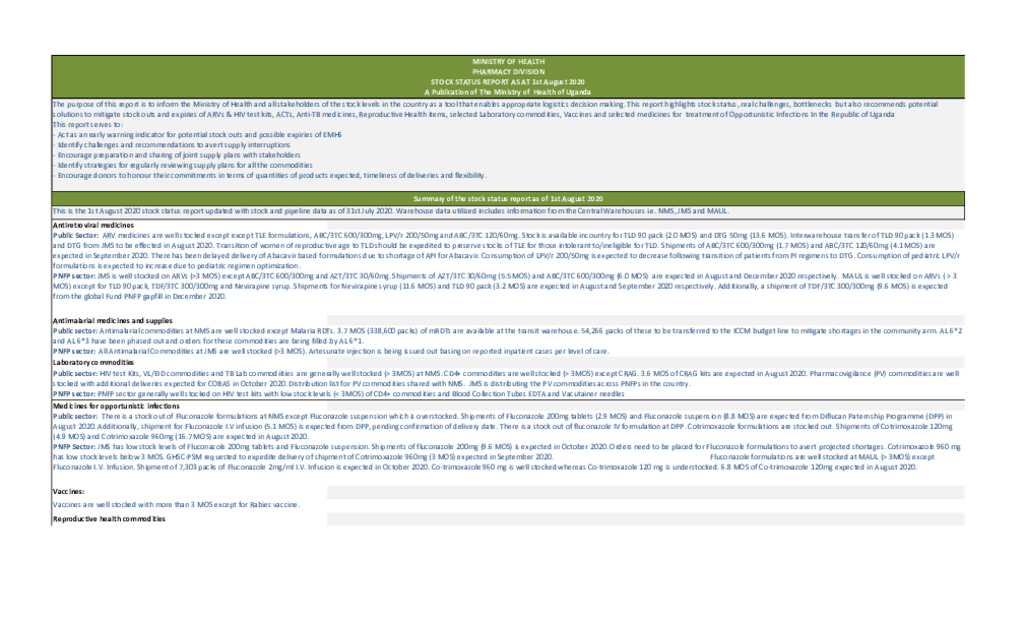
Public Sector: ARV medicines are well stocked except except TLE formulations, ABC/3TC 600/300mg, LPV/r 200/50mg and ABC/3TC 120/60mg. Stock is available incountry for TLD 90 pack (2.0 MOS) and DTG 50mg (13.6 MOS). Interwarehouse transfer of TLD 90 pack (1.3 MOS) and DTG from JMS to be effected in August 2020. Transition of women of reproductive age to TLD should be expedited to preserve stocks of TLE for those intolerant to/ineligible for TLD. Shipments of ABC/3TC 600/300mg (1.7 MOS) and ABC/3TC 120/60mg (4.1 MOS) are expected in September 2020. There has been delayed delivery of Abacavir based formulations due to shortage of API for Abacavir. Consumption of LPV/r 200/50mg is expected to decrease following transition of patients from PI regimens to DTG. Consumption of pediatric LPV/r formulations is expected to increase due to pediatric regimen optimization. PNFP sector: JMS is well stocked on ARVs (>3 MOS) except ABC/3TC 600/300mg and AZT/3TC 30/60mg. Shipments of AZT/3TC 30/60mg (5.5 MOS) and ABC/3TC 600/300mg (6.0 MOS) are expected in August and December 2020 respectively. MAUL is well stocked on ARVs ( > 3 MOS) except for TLD 90 pack, TDF/3TC 300/300mg and Nevirapine syrup. Shipments for Nevirapine syrup (11.6 MOS) and TLD 90 pack (3.2 MOS) are expected in August and September 2020 respectively. Additionally, a shipment of TDF/3TC 300/300mg (9.6 MOS) is expected from the global Fund PNFP gapfill in December 2020.
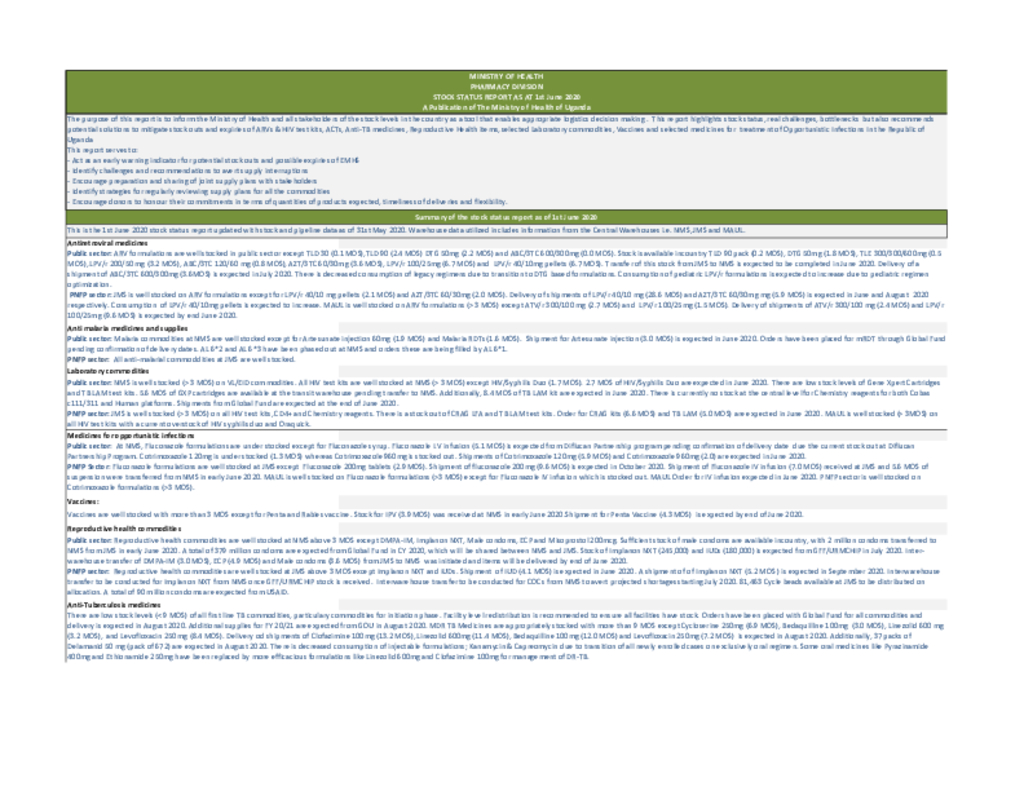
The purpose of this report is to inform the Ministry of Health and all stakeholders of the stock levels in the country as a tool that enables appropriate logistics decision making . This report highlights stock status, real challenges, bottlenecks but also recommends potential solutions to mitigate stock outs and expiries of ARVs & HIV test kits, ACTs, Anti-TB medicines, Reproductive Health items, selected Laboratory commodities, Vaccines and selected medicines for treatment of Opportunistic Infections In the Republic of Uganda This report serves to: - Act as an early warning indicator for potential stock outs and possible expiries of EMHS - Identify challenges and recommendations to avert supply interruptions - Encourage preparation and sharing of joint supply plans with stakeholders - Identify strategies for regularly reviewing supply plans for all the commodities - Encourage donors to honour their commitments in terms of quantities of products expected, timeliness of deliveries and flexibility
The purpose of this report is to inform the Ministry of Health and all stakeholders of the stock levels in the country as a tool that enables appropriate logistics decision making . This report highlights stock status, real challenges, bottlenecks but also recommends potential solutions to mitigate stock outs and expiries of ARVs & HIV test kits, ACTs, Anti-TB medicines, Reproductive Health items, selected Laboratory commodities, Vaccines and selected medicines for treatment of Opportunistic Infections In the Republic of Uganda This report serves to: - Act as an early warning indicator for potential stock outs and possible expiries of EMHS - Identify challenges and recommendations to avert supply interruptions - Encourage preparation and sharing of joint supply plans with stakeholders - Identify strategies for regularly reviewing supply plans for all the commodities - Encourage donors to honour their commitments in terms of quantities of products expected, timeliness of deliveries and flexibility.




