This Learner's Guide, Part I of the module on the Diagnosis and Management of Severe Falciparum Malaria, is made up of teaching materials, problems and a picture quiz covering all the activities involved in diagnosing and managing severe falciparum malaria at the hospital level. This guide is based upon the problem solving approach to education, and working through the study cases presented, you will develop the competence to manage correctly cases of severe falciparum malaria.
Together with Part II, the Tutor's Guide, it forms a training module which is designed to be used throughout a formal period of training and provides information, poses practical problems and suggested solutions in a simple, easily understandable form, so as to facilitate local adaptation and translation into local languages.
Welcome to the 27th issue of the Malaria quarterly bulletin, which focuses on the second quarter of 2019. The aim of this bulletin is to inform district, national, and global stake-holders on progress achieved and challenges encountered in malaria control and reduction in Uganda. Most importantly, it is to encourage use of this information at all levels in order to foster im-provement of our efforts and to high-light achievements and create aware-ness for increased resource mobilization& allocation in order to maintain the gains we have achieved.
We present updates on key malaria morbidity, mortality and intervention indicators; Updates from Malaria Reference Centers; 9th End User Verifica-tion Key findings; and updates from NMCP strategic units. We welcome your thoughts and contributions regarding this publication

Reporting rate this week (86.4%) represents change from the previous week, 2019W8 (86.7%). There was a 10% drop reported in malaria cases (106,503 in W8 vs. 95,761 this week. The West Nile districts of Adjumani (13) & Moyo (13) reported incidence rates >10 cases/1,000 population. Further south, Namayingo District also reported incidence rates beyond 10 cases/1,000 population . About 26% (33/128) of districts treated ≥15% of patients who tested negative with an antimalarial. This is a 3%-point increase from 30% in 2019W8. There were 22 deaths this week, representing a 38% increase from last week (16). About 30% (38/128) of districts had reporting rates <85%, representing a 14%-point increase from 2019W9 (16%).
IMAI/IMCI (Integrated Management of Adolescent and Adult Illness/Integrated Management of Childhood Illness) is a multi-departmental project in WHO producing guidelines and training materials for first-level facility health workers in low-resource settings. IMAI/IMCI are part of the WHO model essential package for HIV prevention, care and treatment.
A number of cases have been reported in which people living with HIV have been criminally charged for a variety of acts that transmit HIV or risk transmission. In some cases, criminal charges have been laid for conduct that is merely perceived as risking transmission, sometimes with very harsh penalties imposed. Some jurisdictions have moved to enact or amend legislation specifically to address such conduct. The issue has also received public and academic commentary
Community HIV Counselling and Testing (COHCT) is an approach that utilises existing community competencies in dealing with HIV/AIDS in general, and HIV counselling and testing in particular. The COHCT concept is premised on the knowledge that HIV counselling and testing is an entry point into HIV prevention, care and support and that communities have a primary role to play in the HIV/AIDS intervention. The approach utilises participatory methodologies to engage community members in analysing their HIV/AIDS situation, and, from the existing social mechanisms and structures, identify the options that would enable them mobilise for HCT and thereafter deal with the usual outcomes of HIV test:
Over 2 million children worldwide are living with HIV infection and 95% reside in sub-Saharan Africa with the majority infected through mother-to-child transmission. Infected children have a high mortality with 50% dying by 2 years of age. Their clinical presentation includes common childhood infections, opportunistic infections and conditions associated with HIV/AIDS immune suppression.
This document provides guidance to countries on what actions need to be taken when countries consider changing their national policy for the first-line treatment for malaria to an ACT consistent with WHO recommendations. It addresses operational and technical considerations for both the public and private sectors, and it may be used as a planning tool to identify technical assistance and resource needs. This document focuses on the implementation process after a decision is made to change the
treatment policies. Some documents providing guidance on achieving the policy change are listed in Annex 4.
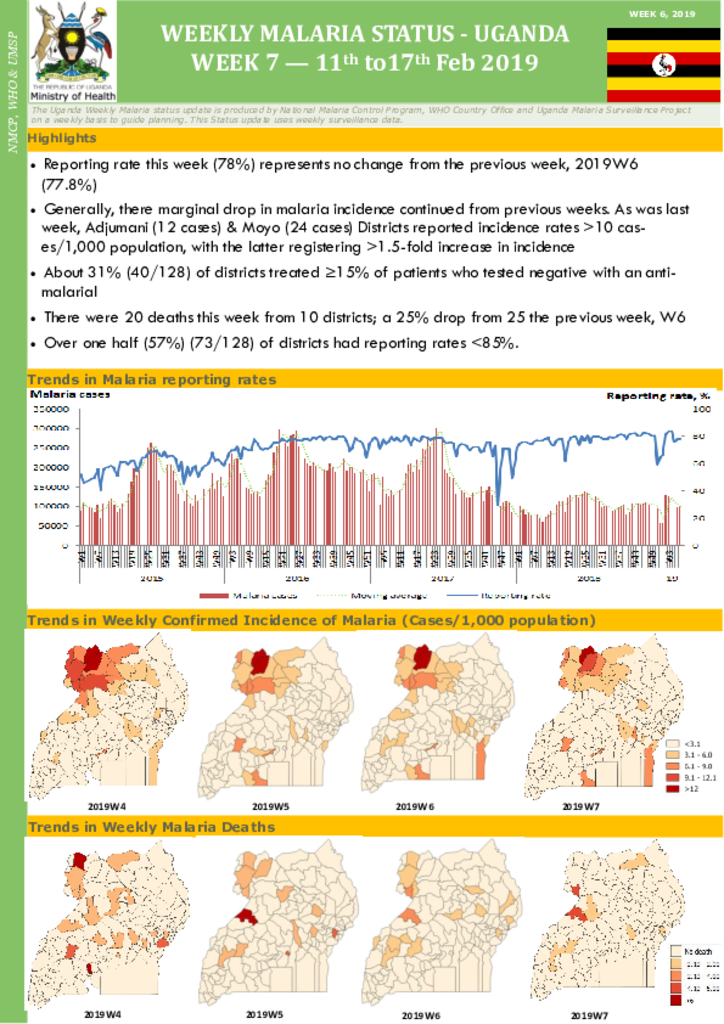
Reporting rate this week (78%) represents no change from the previous week, 2019W6 (77.8%) Generally, there marginal drop in malaria incidence continued from previous weeks. As was last week, Adjumani (12 cases) & Moyo (24 cases) Districts reported incidence rates >10 cas-es/1,000 population, with the latter registering >1.5-fold increase in incidence. About 31% (40/128) of districts treated ≥15% of patients who tested negative with an anti-malarial. There were 20 deaths this week from 10 districts; a 25% drop from 25 the previous week, W6. Over one half (57%) (73/128) of districts had reporting rates <85%.
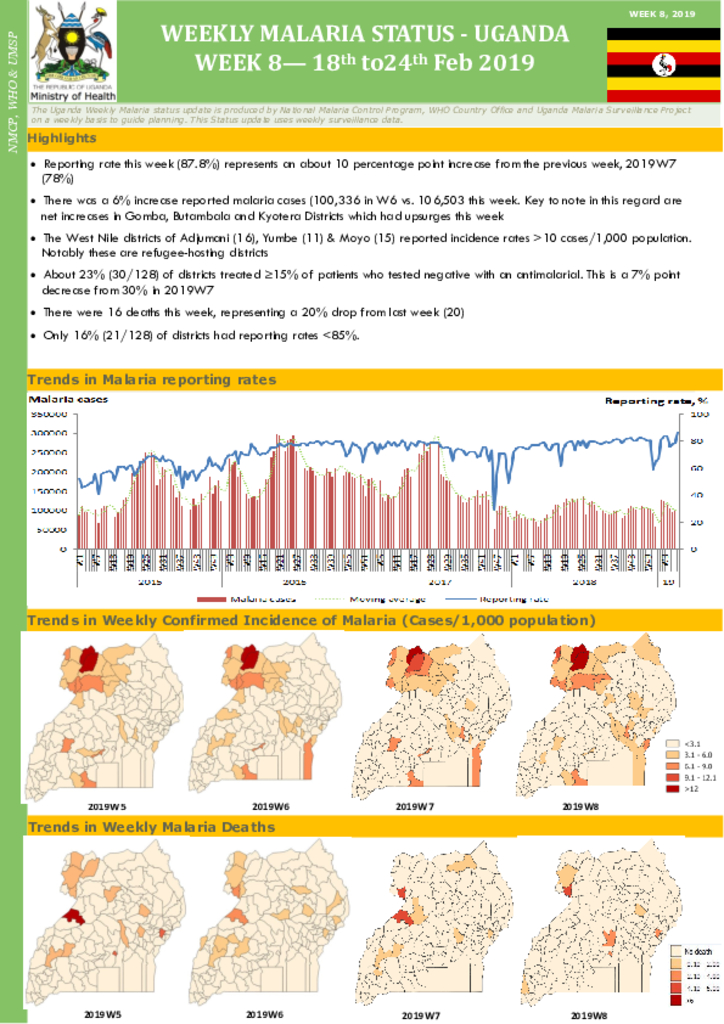
Reporting rate this week (87.8%) represents an about 10 percentage point increase from the previous week, 2019W7 (78%) There was a 6% increase reported malaria cases (100,336 in W6 vs. 106,503 this week. Key to note in this regard are net increases in Gomba, Butambala and Kyotera Districts which had upsurges this week The West Nile districts of Adjumani (16), Yumbe (11) & Moyo (15) reported incidence rates >10 cases/1,000 population.Notably these are refugee-hosting districts About 23% (30/128) of districts treated ≥15% of patients who tested negative with an antimalarial. This is a 7% point decrease from 30% in 2019W7 There were 16 deaths this week, representing a 20% drop from last week (20) Only 16% (21/128) of districts had reporting rates <85%.
Uganda was one of the first sub-Saharan countries to be affected by the Human immunodeficiency virus (HIV) epidemic. The first Acquired immune deficiency syndrome (AIDS) case reported in the country was recognized in 1982. Following this report, efforts were mounted to deal with the epidemic. The efforts amongst others included an open policy in managing the HIV/AIDS epidemic declared by the National Resistance Movement Government after it assumed power in 1986. Since then, there has been high-level political and donor support backed by resources for AIDS control. The Multi-Sectoral AIDS Control Approach (MACA) and the National Operation Plan reflected the recognition by the Government and civil society of the need to scale up a multi-faceted and multisectoral response from all sectors of the government and society.

Reporting rate this week (83.9%) was similar to that in the previous week, 2019W2 (83.6%).There was a 7.2% drop in reported malaria cases (125,427 in W3 vs. 116,330 cases this week). Adjumani, Nwoya & Moyo Districts reported the highest confirmed incidence rates ≥15 cases/1,000 population. Almost half (61/128) of districts treated ≥5% of patients who tested negative with an antimalarial
There were 34 deaths this week from 22 districts. About 43% of districts had reporting rates less than 85%. This is a 27%-point improvement compared to 70% in the previous week, 2019W3




